
2.12: Canalplasty and Exostosis
- Page ID
- 17710

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
CANALPLASTY FOR EXOSTOSIS
Loren Britto & Thomas Linder
Definition of Exostosis
Exostosis is an abnormal benign bony growth within the external ear canal. It is frequently multiple and bilateral and is very common in individuals with repeated exposure to cold water and wind. Patients may develop conductive hearing loss and/or recurrent ear infections due to trapped water and earwax between the tympanic membrane and the exostosis.
Indications for Canalplasty
Retention of cerumen and keratin in the external ear canal (EAC) associated with recurrent episodes of external otitis.
Preoperative assessment
Otomicroscopy

Figure 1: Multiple exostoses

Figure 2: Exostoses
The findings are partial or total obstruction of the bony external ear canal and retention of cerumen. In some cases it is not possible to visualize the eardrum at all. It is important to assess the cartilaginous entrance to the ear canal in order to plan for a meatoplasty at a later stage (Figures 1, 2).
Audiometry
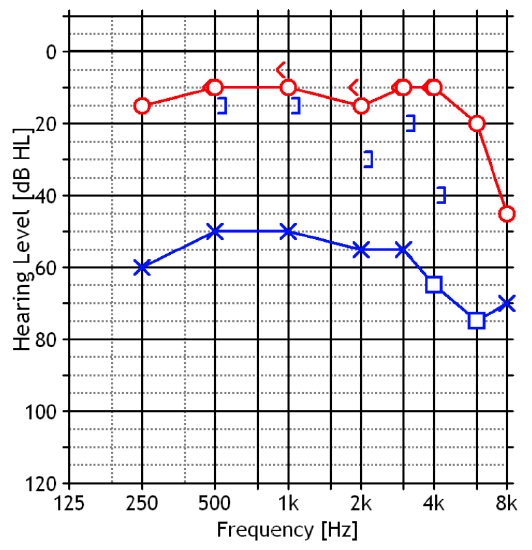
Figure 3: Conductive hearing loss in the left ear
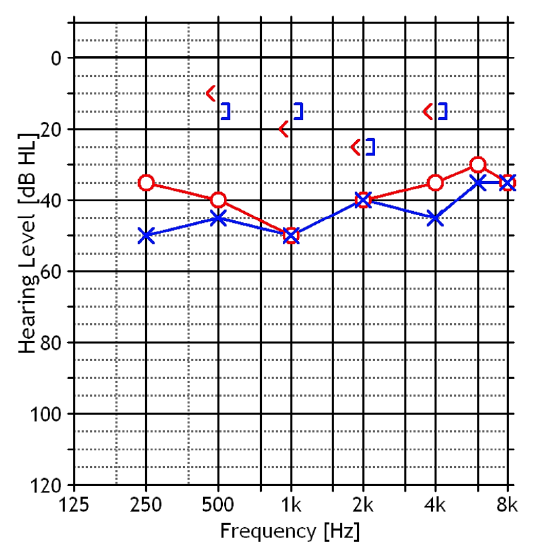
Figure 4: Bilateral conductive hearing loss
The audiogram may be normal in case of partial obliteration or may reveal a conductive hearing loss in cases of complete or almost total exostoses with retention of cerumen (Figures 3, 4).
Imaging
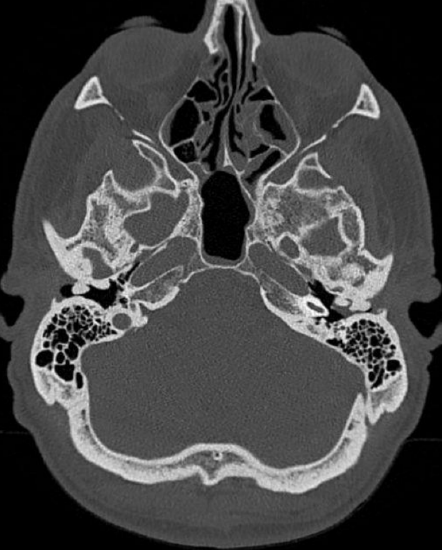
Figure 5: Multiple, bilateral exostoses with retention of cerumen on the left side
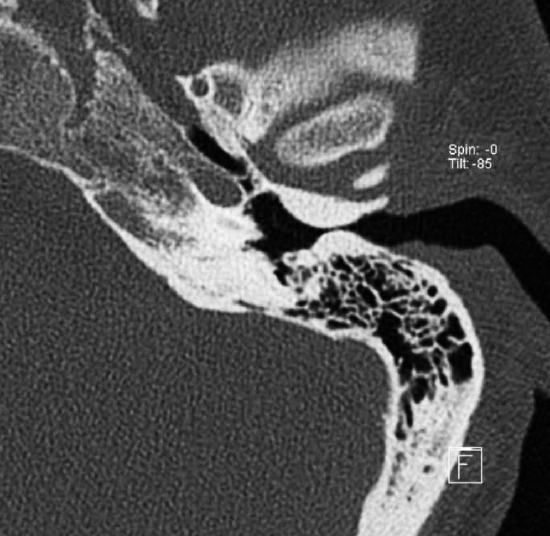
Figure 6: Axial CT scan of left ear with anteroposterior exostoses without retention of cerumen
CT scan shows the extent of the exostoses and helps the surgeon to determine the amount of bone that needs to be removed and avoiding injuries to nearby structures (Figures 5, 6).
Surgical Principles
- Removal of external canal exostoses requires complete elimination of the overhanging bone lateral to the tympanic annulus
- The meatal skin should be kept intact and vital to promote rapid reepithelization following enlargement of the bony ear canal
- With a narrow ear canal entrance, meatoplasty is combined with the canalplasty, removing the excess conchal cartilage and subcutaneous tissue, thereby yielding a large cartilaginous external canal that ensures excellent visibility of the exostotic posterior canal
- In cases of severe bilateral exostosis, wait three months to operate on the other side
Surgical Approaches
The pathology can be addressed by an endaural or a retroauricular approach. The endaural approach is well suited to less severe exostoses and for surgeons who are familiar with endaural approaches for other pathologies. Less experienced surgeons may favor a retroauricular approach as the exposure is more familiar to them and there is a wider field of action.
Endaural Approach
General Considerations
Although the surgery can be performed under local anesthesia with sedation, we prefer general anesthesia due to the uncomfortable drilling noise. Antibiotic prophylaxis is not required.
Surgical Steps (left ear)
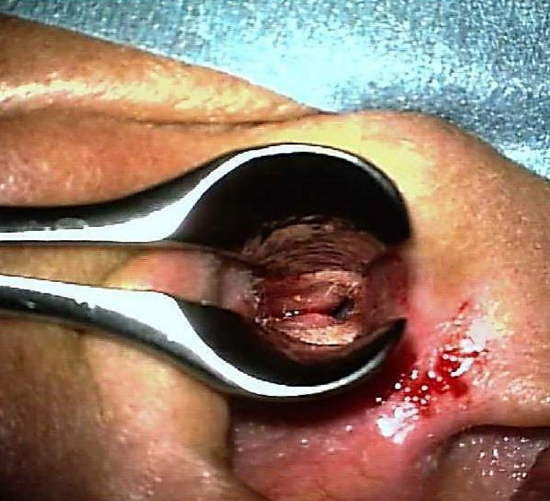
Figure 7: Speculum aiding infiltration
- Infiltrate the site of the endaural skin incision as well as the ear canal in 4 quadrants with local anesthetic (lidocaine 1% & adrenaline diluted to 1:200 000) (Figure 7)
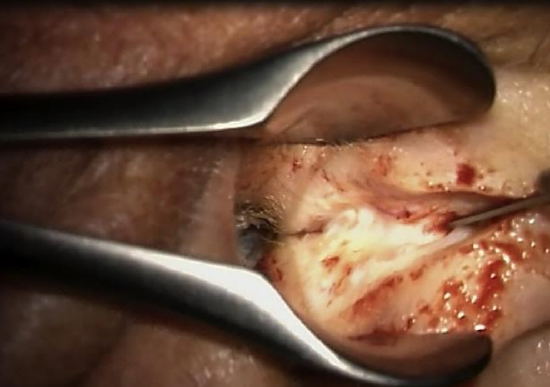
Figure 8: Helicotragal incision
- Using a nasal speculum, make a helicotragal incision with a #15 blade and (Figure 8)

Figure 9: Posterior incision
- Make a posterior semicircular incision over the edge of the exostosis, meeting the endaural incision at 12 o’clock (Figure 9)
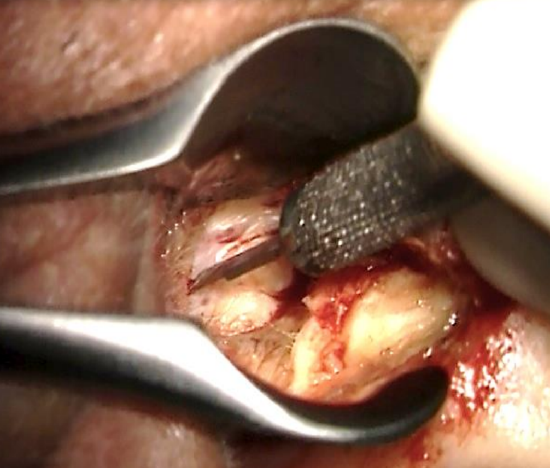
Figure 10: Prolong the posterior incision
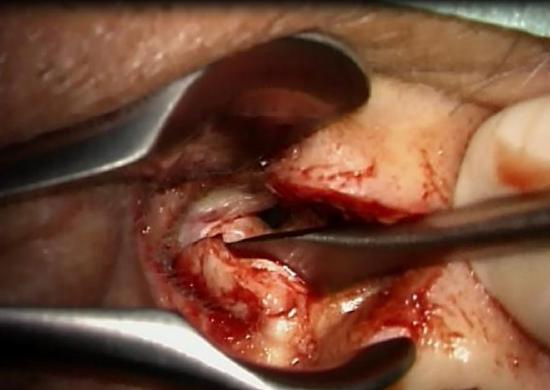
Figure 11: Reflect posterior skin laterally
- Prolong the inferior part of the incision posteriorly and reflect the posterior skin laterally (Figures 10, 11)
- Enlarge the entrance of the canal with two Fisch endaural retractors
- An anterior semicircumferential incision is made along the lateral margin of the anterior exostosis
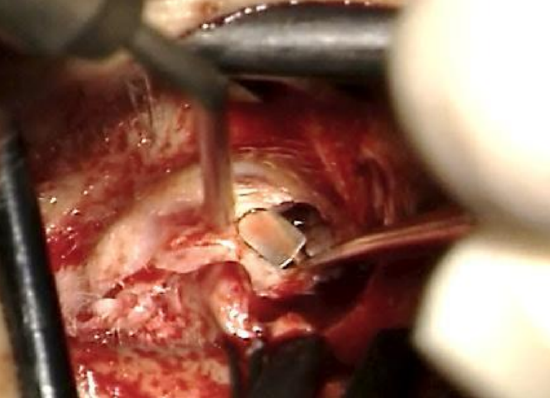
Figure 12: Elevate anterior skin laterally

Figure 13: Elevate anterior skin laterally
- Reflect the anterior canal skin and soft tissue laterally using a Fisch or Iowa microraspatory and a Key raspatory. A round knife may also be used, but will get blunt when dissecting on bone (Figures 12, 13)
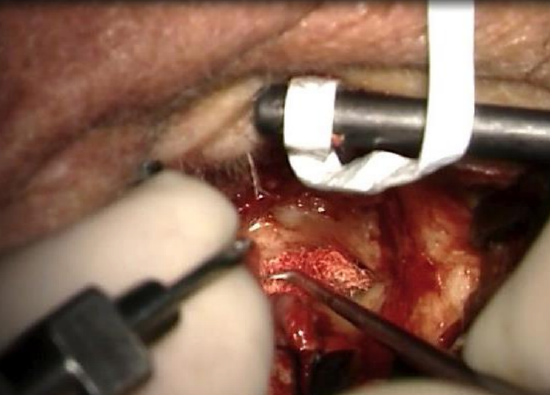
Figure 14: Elevate skin with Fisch microraspatory and adrenaline gauze
- The anterior skin flap is kept elevated and retracted from the lumen with an aluminium strip anchored to the Fisch endaural retractor (Figure 14)
- Elevate the skin over the exostotic bone using microraspatories and small gauze strips (1-1.5 cm in length) soaked in adrenaline solution. The gauze strips allow careful dissection between skin and bone and avoid lacerations to the skin flaps (Figure 14)
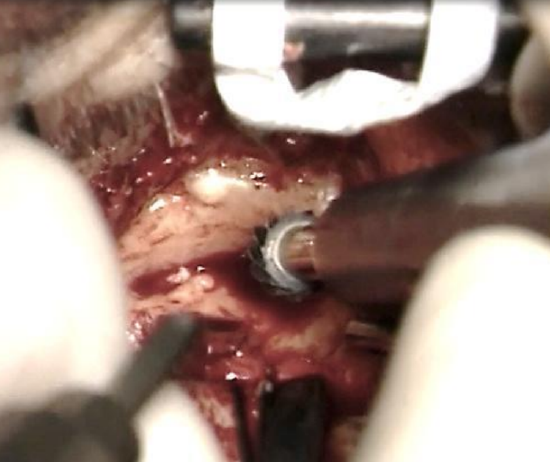
Figure 15: Sharp burr
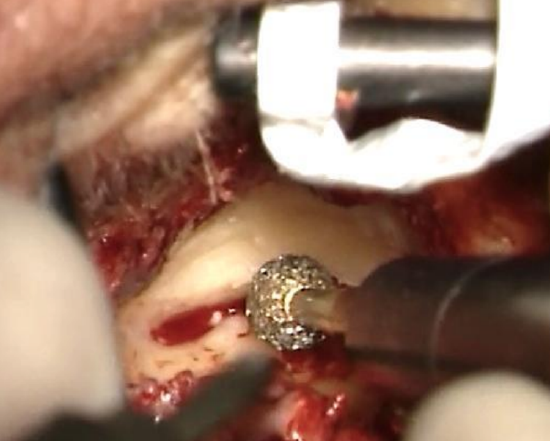
Figure 16: Diamond burr
- Remove the excess bone along the canal wall. A sharp drill is only used at the outer entrance to the bony ear canal far away from the skin flaps. Once the dissection proceeds into the bony ear canal, diamond burrs are used. (Figures 15, 16)
- Since preservation of the ear canal skin is vital to allow proper wound healing, the following steps and tricks are helpful to achieve this goal:
- The left hand (for right-handed surgeon) cleans the field holding otosclerosis suction tips and assists the right hand while drilling
- Continuous irrigation is mandatory to see any color changes within the bone (appearance of temporomandibular joint anteriorly or mastoid air cells posteriorly)
- To protect the skin from damage, a groove or sulcus is made in the exostosis, leaving a thin layer of bone covering the elevated skin. Avoid drilling on the edge; always stays behind the edge of the groove/sulcus. The outer limits are the temporomandibular joint anteriorly and the mastoid air cells posteriorly

Figure 17: Skin protected

Figure 18: Elevating skin with adrenaline gauze

Figure 19: Checking vitality of the skin

Figure 20: A groove is made, and the skin left protected medially
- Elevate the skin with an adrenaline gauze, leaving the skin safe medial to the edge of bone (Figures 17-20)
- Drilling should be discontinued if a bluish color in the bone is noted anteriorly while irrigating to avoid entering the temporomandibular joint

Figure 21: Silastic sheet
- Approaching the eardrum, drill at the edge, using a silastic sheet to protect the skin (Figure 21)
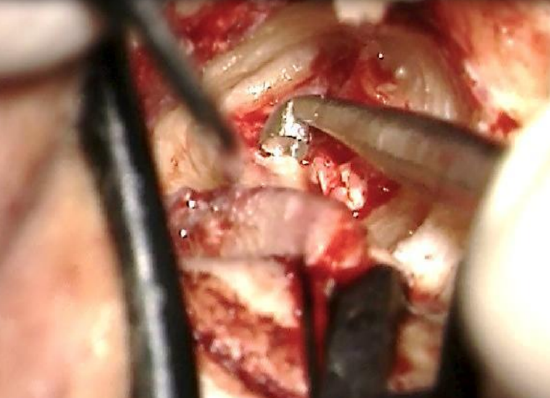
Figure 22: Curetting bone over annulus

Figure 23: Curetting bone over annulus
- When the tympanic annulus appears through the posterior side of the flap, the eggshell of bone protecting the meatal skin is removed with a Fisch microraspatory and curette (Figures 22, 23)
- The EAC is shaped into an inverted truncated cone
- Correct widening of the EAC requires elimination of all overhanging bone lateral to the tympanic annulus. Failure to open the tympanomeatal angle at the level of the annulus causes accumulation of keratin with recurrence of the exostoses
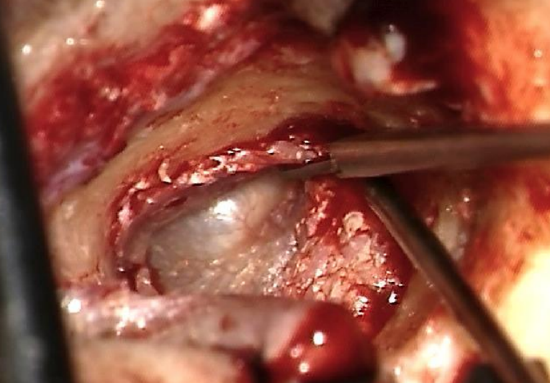
Figure 24: Incising at 1 & 5 o’clock

Figure 25: Incising at 1 & 5 o’clock
- The flap of ear canal skin is placed back in position. Releasing cuts are made at 11 and 7 o’clock (right ear) to accommodate the skin properly on the new bone canal (Figures 24, 25)
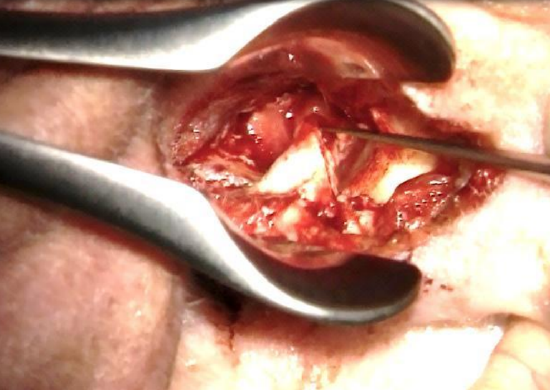
Figure 26: Repositioning posterior meatal skin and covering it with gelfoam

Figure 27: Positioning the gelfoam
- The meatal skin flap is repositioned and covered with Gelfoam pledgets soaked in corticosporin (Figures 26, 27)
- The endaural incision is closed with 3/0 Vicryl and 4/0 Prolene sutures
Retroauricular Approach
This approach allows better visualization of the canal.
Indications
- Total exostosis without lumen
- Less experienced surgeon (better landmarks, larger operative field, same outcome)
General Considerations
The surgery is performed under general anesthesia (local anesthesia is possible, but noise of drilling burr can be difficult for the patient to accept). Antibiotic prophylaxis is not required.
Surgical Steps (Left ear)
- Using local anesthetic (lidocaine 1% and adrenaline diluted to 1:200 000), infiltrate the postauricular sulcus. Then advance the needle and infiltrate the tissues anteroinferiorly and anterosuperiorly
- Use a Lempert’s speculum to visualize the bony-cartilaginous junction and injecting the 4 quadrants of the skin of the ear canal

Figure 28: Posterior incision

Figure 29: Extending the posterior incision inferiorly
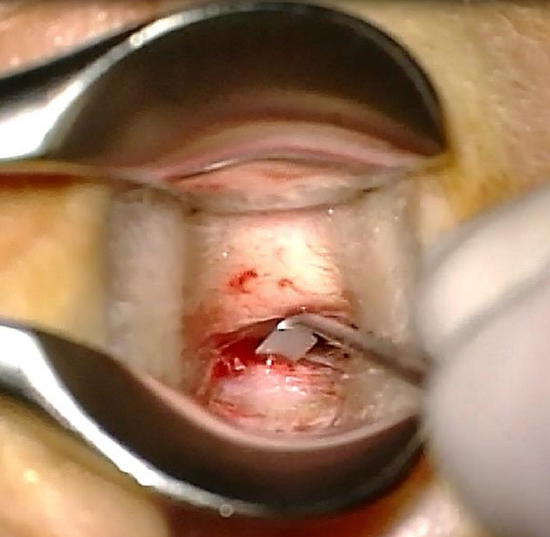
Figure 30: Reflecting the posterior flap
- Using a Lempert’s speculum, make a posterior transcanal incision over the edge of the exostosis, with an inferior extension. Reflect the skin flap laterally (Figures 28-30)

Figure 31: Retroauricular skin incision
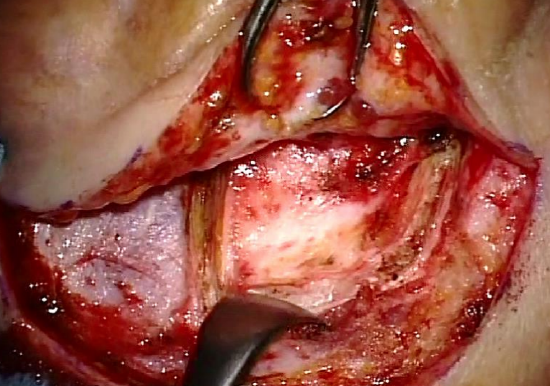
Figure 32: Periosteal flap
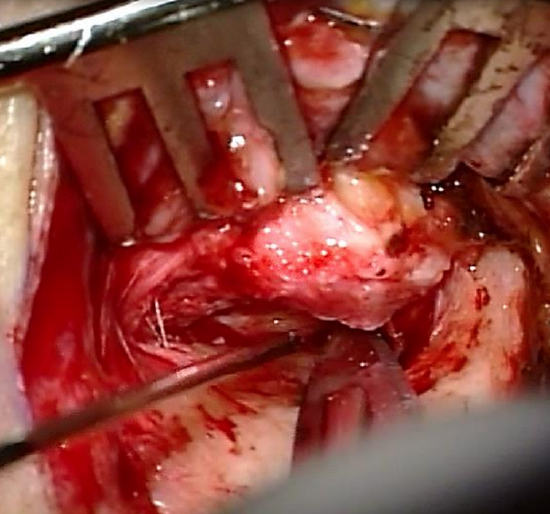
Figure 33: Anterior incision
- Start the retroauricular approach like for tympanoplasty (Figures 32, 33) (Myringoplasty & tympanoplasty chapter)
- The end of the periosteal flap elevation meets the posterior transcanal incision
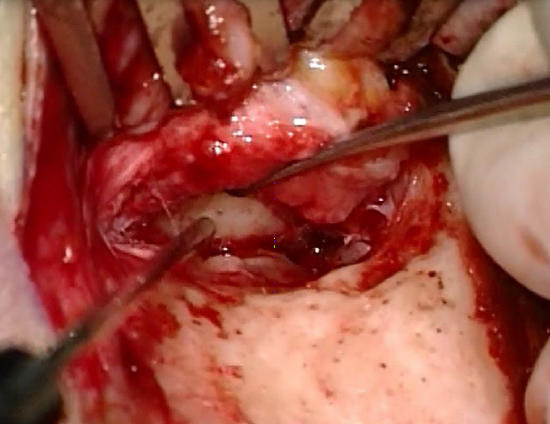
Figure 34: Reflecting the anterior skin flap laterally
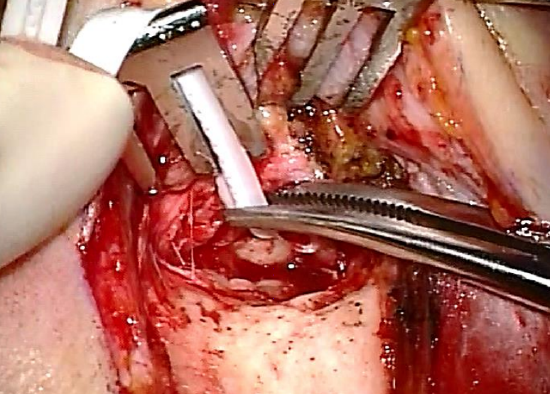
Figure 35: Aluminium strip
- Incise the anterior canal wall with an #11 blade and reflect the skin laterally. Keep the anterior skin out of the surgical field with an aluminium strip (Figures 33-35)
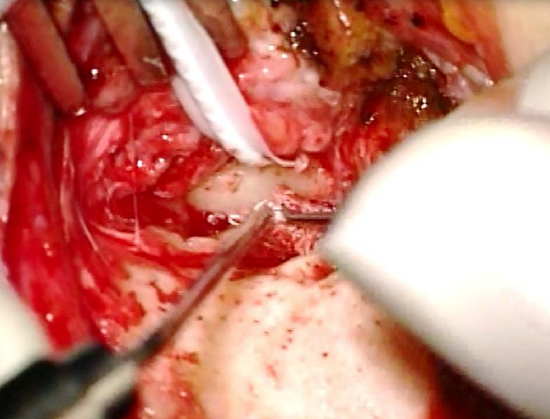
Figure 36: Elevating canal skin with Fisch microraspatory and adrenaline gauze
- Perform the next steps as for Endaural approach (Figure 36)
- Cover the skin with Gelfoam pledgets soaked in corticosporin
- Suture the retroauricular incision with 3-0 Vicryl and 4-0 Prolene
Videos
Exostosis surgery: Endaural approach
Exostosis surgery: Retroauricular approach
Author
Loren Britto M.D.
Fisch Instrument Microsurgical Fellow
Lucerne Canton Hospital, Switzerland
lorenbritto@uol.com.br
Senior Author
Thomas Linder, M.D.
Professor, Chairman and Head of Department of Otorhinolaryngology, Head, Neck and Facial Plastic Surgery
Lucerne Canton Hospital, Switzerland
thomas.linder@ksl.ch
Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za