
1.11: Lipid Lowering Drugs - Hyperlipidemia and Atherosclerosis
- Page ID
- 10632

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Atherosclerosis: A chronic inflammatory disease characterized by enzymatic destruction of the normal arterial skeleton (largely elastin, collagen and smooth muscle), and replacement by disorganized collagen and elastin, cholesterol, and foam cells.
- Afflicts all long-lived mammals.
- Major risk factors:
- Longevity
- Hypertension
- Diabetes – glycosylation of plasma proteins and arterial wall proteins
- Dyslipoproteinemia
- Cigarette Smoking
- Homocysteinemia
- Plasma homocysteine levels controlled by 3 genes related to methionine metabolism
- High homocysteine is toxic to the endothelium and eventually atherogenic
- Lp(a) lipoprotein
- Levels variable and genetically determined
- Inhibits tissue plasminogen activator and allows thrombus formation, which may be atherogenic
- Increases likelihood of thrombosis and clinical catastrophe when atherosclerosis is present
- Chronic bacterial infection
- Transmembrane Receptors on Mammalian Cells – Three Broad Classes
- Receptors mediating transmembrane signaling (e.g. β receptor)
- Serve to amplify the effect of a tiny concentration of ligand
- Receptors regulating intracellular substrate concentration (e.g., LDL receptor)
- Bind tiny fraction of substrate
- Rapid cholesterol turnover involves translocation into the cell
- Receptors supply cholesterol, when needed, to rapidly growing cells
- Normally strongly down-regulated except in liver
- Scavenger receptors (e.g., asialoglycoprotein receptor)
- Receptors of normal catabolism
- Remove certain “worn out” proteins from the plasma or extracellular fluid.
- Oldest of these, the asialoglycoprotein receptor, was described more than 30 years ago. Removes liver proteins which have become desialated over time from the plasma.
- Recently, more scavenger receptors described which scavenge oxidized albumin, oxidized LDL, and many others
- SR-B1 is the HDL scavenger receptor
- Receptors mediating transmembrane signaling (e.g. β receptor)
- Apolipoproteins
- Proteins involved in the solubilization of fat for transport into and out of cells, from one place in the body to another.
- Many types, but most important are A1, B, and E
- All three involved in cholesterol transport
- A1 and B in triglyceride as well
- ApoE has 3 common variants. Plays a critical role in cholesterol absorption, reverse cholesterol transport, and in inhibiting the accumulation in cells of certain hydrophobic proteins.
- Sterols
- Distinguishing feature between plants and animals is not the presence or absence of chlorophyll, but rather the sterols they synthesize.
- Major plant sterol is sitosterol
- Major animal sterol is cholesterol
- Animals differ widely in how they absorb and excrete sterols.
- Disease sitosterolemia highlights importance to human health of sterol absorption and excretion.
- Multiple sterol pumps regulate cellular and body sterol concentrations. These are energy-requiring ATP-dependent pumps.
- ABC (ATP Binding Cassette) transporter family (recently discovered)
- ABCA1 is a reverse cholesterol transporter in all cells. Defect causes Tangier disease (inherited HDL deficiency)
- ABC5 and 8 are proteins which mediate sterol absorption by gut and sterol secretion by liver cells.
- Distinguishing feature between plants and animals is not the presence or absence of chlorophyll, but rather the sterols they synthesize.
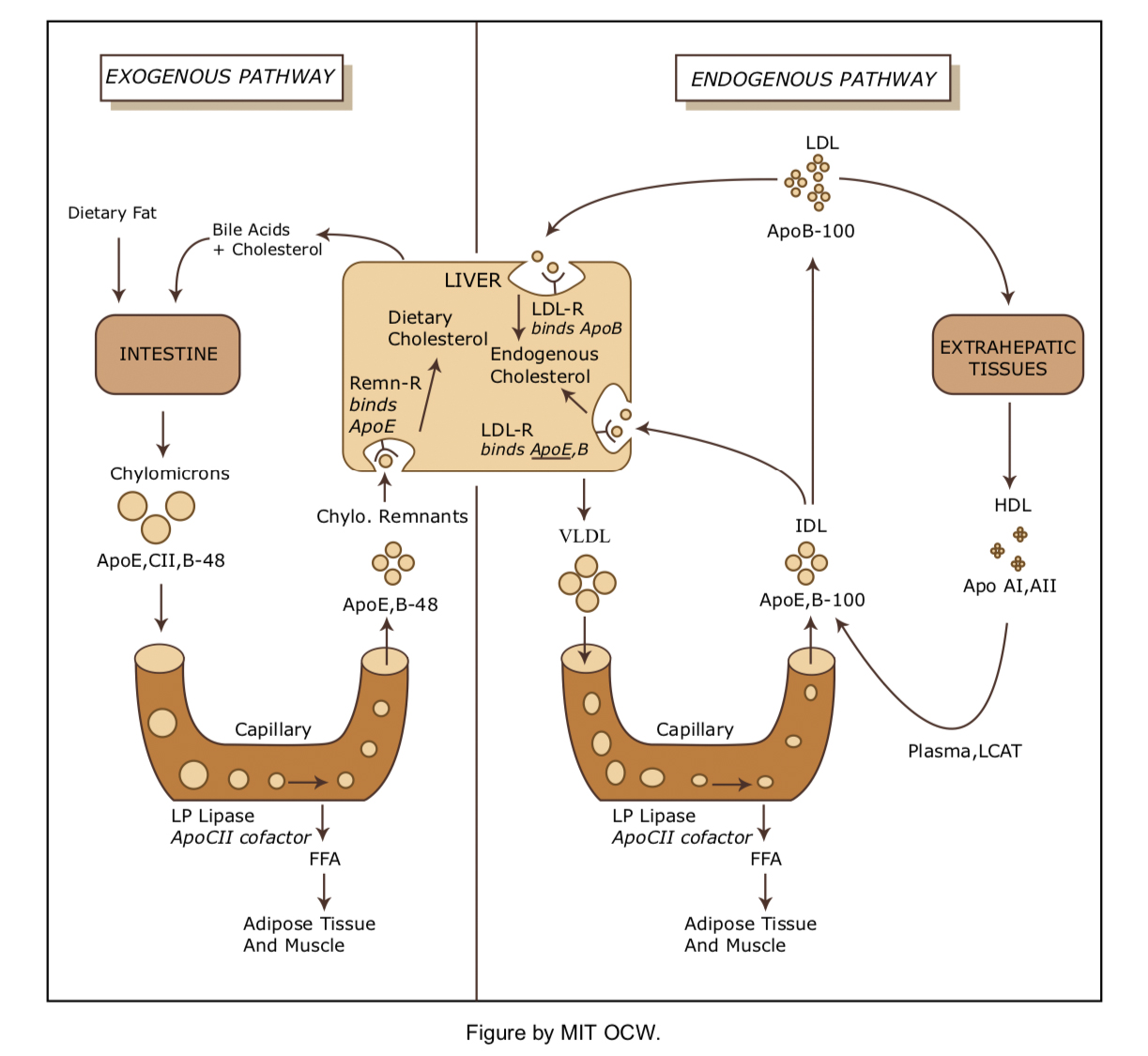
- Exogenous Lipid Transport
- Cholesterol is variably absorbed in the small intestine and incorporated into chylomicrons by the gut mucosal cells.
- Hydrophobic core = triglyceride (95%) + esterified cholesterol.
- Amphipathic surface = Phospholipids, non-esterified cholesterol, and apolipoproteins (B48, C, E, A-I, A-II).
- Chylomicrons travel via the lacteals and the thoracic duct to the venous circulation.
- In muscle and adipose cells the triglyceride core is progressively hydrolyzed by hormone sensitive lipase (HSL) to form free fatty acids. This leaves a so-called chylomicron remnant. (Apo C obtained from circulating HDL is required for this step.)
- Apo A and C are then removed and recycled to HDL, and the chylomicron remnants are taken up by hepatocytes. This process involves LDL receptor-mediated endocytosis and requires Apo E.
- The liver may now excrete the cholesterol into bile (either unchanged or as bile acids), incorporate it into membranes, or resecrete it into plasma as lipoprotein cholesterol.
- Cholesterol is variably absorbed in the small intestine and incorporated into chylomicrons by the gut mucosal cells.
- Endogenous Lipid Transport: The VLDL-LDL Cycle (Apo B100 System)
- This cycle allows the hepatocyte to export triglycerides and cholesterol to peripheral tissues as VLDL. VLDL synthesis requires microsomal triglyceride transfer protein (MTP).
- Hydrophobic core = triglycerides (55-80%) + esterified cholesterol (5- 15%)
- Surface = phospholipids (10-20%), Apo B100, C, E
- The triglycerides in hepatocytes come from two sources:
- FFA synthesized de novo in liver
- FFA and glycerol taken up from plasma and re-esterified. These are produced in adipose tissue and muscle by the action of HSL. HSL activity is regulated by adrenergic nerves and circulating catecholamines.
- The cholesterol in hepatocytes also comes from two sources
- Uptake of chylomicron remnants
- Synthesized de novo by HMG CoA-reductase
- Once the VLDL are circulating, the triglycerides may be hydrolyzed by HSL in plasma, and the fatty acids may be used to provide fuel for muscle cells, or re- esterified and stored in adipocytes. When the VLDL particle has been depleted of triglycerides it becomes a smaller, denser particle called a VLDL remnant orIDL.
- Like chylomicron remnants, the triglyceride-poor VLDL remnants may reenter the liver. Unlike chylomicrons, the VLDL remnants may be further metabolized to become LDL.
- The major determinant of LDL concentration in plasma is the number/activity of LDL receptors.
- Present on nearly all cells and account for 70-80% of LDL catabolism.
- Most LDL taken up by liver and the rest by peripheral tissues, adrenals and gonads (the latter need cholesterol for steroid synthesis).
- Apo E is critical ligand for binding of lipid particles to LDL receptor
- This cycle allows the hepatocyte to export triglycerides and cholesterol to peripheral tissues as VLDL. VLDL synthesis requires microsomal triglyceride transfer protein (MTP).
- Endogenous Lipid Transport: The HDL Cycle (Apo A-I System)
- This “antiatherogenic” cycle allows cholesterol to be scavenged from chylomicrons, VLDL and peripheral tissues by HDL particles.
- Core = triglycerides (5-10%) + esterified cholesterol (15-25%)
- Surface = phospholipids, + Apo A-I, A-II, C, E
- Transport of cholesterol from tissue stores to HDL is mediated by ABCA1transporter. It is then esterified by lecithin-cholesterol acyltransferase (LCAT)to make bigger HDL particles. Esterified cholesterol is then disposed of by three primary mechanisms:
- Transfer to VLDL, LDL, IDL, and chylomicron remnants by cholesteryl ester transfer protein (CETP) and subsequent endocytosis by hepatocytes.
- Direct uptake in liver, adrenals, and gonads by the scavenger HDL receptor called SR-BI.
- Hydrolysis by hepatic lipase
- This “antiatherogenic” cycle allows cholesterol to be scavenged from chylomicrons, VLDL and peripheral tissues by HDL particles.
- Exogenous Lipid Transport
- Lipid Lowering Drugs
- HMG-CoA Reductase Inhibitors: Statins
- Mechanism of Action: Structural analogs of 3-hydroxy-3-methylglutaric acid (HMG) that competitively inhibit HMG-CoA reductase, the rate-limiting step in cholesterol synthesis.
- Endogenous Regulation: Hepatocytes maintain critical intracellular sterol pools. The genes for HMG-CoA reductase and the LDL receptor are under the transcriptional control of an SRE (sterol responsive element). When enough sterol is present in the cell, a repressor binds to the SRE inhibiting the transcription of enzyme and receptor and thus the production and recycling of more cholesterol.
- Physiologic Response to HMG-CoA Reductase Inhibitors: By inhibiting cholesterol production, statins deplete sterol pools, “activating” the production of HMG-CoA reductase and the LDL receptor. The increase in LDL receptor levels results in the uptake of more IDL and LDL from the plasma. The net effect is that a new steady state is established with lower levels of plasma LDL. The most effective statins, such as atorvastatin and rosuvastatin can lower LDL by 60-70%.
- It is thought that apoB-100 synthesis (requisite for VLDL) may also be inhibited resulting in decreased VLDL production. This may be one factor that explains the fall in triglycerides from 10% to 30%.
- Usage: Statins are useful agents in all hyperlipidemias (except for homozygous LDL-R deficiency)
- Adverse Effects:
- Co-administration with triazole antifungals, and certain other drugs can virtually arrest cholesterol synthesis, but produces severe toxicity.
- As a group, the statins are quite tolerable with rare serious adverse effects. Some of those effects can include rhabdomyolysis and liver abnormalities.
- Bile Acid Binding Resins: Cholestyramine, Colestipol,
- Mechanism of Action: These are anion exchange resins that are not absorbed by the intestine. They exchange chloride anions for negatively charged bile acids. This results in increased excretion of bile acids.
- Physiologic Response to Bile Acid Binding Resins: Since fewer bile acids are recycled, hepatocytes increase conversion of cholesterol to the production of bile acid. Again this depletes the intracellular sterol pool leading to upregulation of cholesterol synthesis enzymes and LDL receptor. Thus, hepatocyte pools are replenished as a result of increased production of cholesterol as well as enhanced uptake of LDL from plasma. A new steady state is reached with 10-25% less plasma LDL.
- Usage: Resins are useful generally in hyperlipidemia (again except for homozygous LDL-R deficiency).
- Adverse Effects: Since these agents are not absorbed, they are very safe. Gastrointestinal side effects include bloating, constipation, and abdominal discomfort. They also interfere with the absorption of many other drugs, although this problem can be minimized by appropriate timing of drug administration.
- Cholesterol absorption inhibitors: Sitostanol-ester margarine, Colesevelam, Ezetimibe
- Mechanism of Action: Sitostanol-ester margarine is created by saturating the B-ring of sitosterol to produce sitostanol and then esterifying it. Colesevelam is a non-absorbed synthetic soluble fiber. These agents inhibit cholesterol absorption by unknown mechanisms. Ezetimibe is thought to inhibit ABC sterol pumps in gut and liver, reducing the absorption of cholesterol and increasing its secretion into bile. It is absorbed and glucuronidated and undergoes enterohepatic recirculation.
- Physiologic response: All of these drugs lower LDL by 10-15%. None has much effect on HDL or triglycerides.
- Usage: The margarine is available over the counter. The other drugs are prescribed most often as adjunctive therapy. Ezetimibe is marketed in a combination product with simvastatin. The combination has additive effects, so a large decrease in LDL occurs with a lower dose of statin.
- Adverse effects: Almost none.
- Niacin (Nicotinic Acid, Vitamin B3)
- Mechanism of Action and Physiologic Response: Niacin inhibits HSL in adipose tissue. This decreases the levels of free fatty acids in the plasma and the amount delivered to hepatocytes. As a result, less VLDL and triglycerides are synthesized. The reduction in plasma VLDL leads to a 10-15% decrease in LDL. Niacin also produces substantial increases in HDL, probably by decreasing the clearance of its major apolipoprotein, apoAI. Niacin is the only known lipid-lowering agent that has been reported to decrease Lp(a) levels.
- Usage: This drug can produce a long-term improvement in both cardiovascular and total death rate. Niacin is very inexpensive and extremely useful for many patients. A multitude of annoying and occasionally dangerous side effects keep it from being a first-line agent for many.
- Adverse Effects: Cutaneous flushing, headaches, pruritis, dermatitis. Some effects can be decreased by pretreatment with NSAIDs or use of sustained- release preparations. Niacin can cause hyperglycemia (and sometimes overt diabetes), hyperuricemia or gout, gastritis and GI bleeding. Serious liver abnormalities can occur when the drug is taken in large doses.
- Fibric Acid Derivatives: Gemfibrozil and fenofibrate
- Mechanisms of Action and Physiologic Response: These agents stimulate the nuclear receptor peroxisome proliferator-activated receptor α, increasing the expression of many proteins involved in lipid metabolism. They stimulate HSL in muscle and thus, catabolism of triglyceride rich lipoproteins such as VLDL. This can lower the level of triglycerides in the plasma by as much as 35%. Fibrates have also been reported to decrease production of VLDL in hepatocytes by inhibiting fatty acid synthesis. The decrease in VLDL usually leads to some decrease in LDL.
- Fibrates can increase increase HDL levels by 15-25%. This is due to both an increase in HDL production and an increase in reverse cholesterol transport.
- Usage: These drugs are used for hypertriglyceridemia, especially when HDL is low. They are also used in familial dysbetalipoproteinemia.
- Adverse Effects: GI distress, cholelithiasis, myositis, and interaction with warfarin and other albumin bound drugs.
- HMG-CoA Reductase Inhibitors: Statins
- Non-drug Treatment: LDL apheresis
- Two systems for selective removal of LDL from plasma by vein to vein apheresis in U.S. market
- Highly effective in lowering LDL, even with homozygous LDL receptor deficiency.
- Produces arrest and regression of both xanthomas and atherosclerosis
- Limited by cost and inconvenience
- Investigational Treatments
- ACAT (acyl cholesterol acyl transferase) inhibitors
- Mechanism of Action: Inhibits the enzyme that esterifies cholesterol for storage in tissues and prevents cholesterol absorption and its storage in arterial foam cells.
- Adverse effects: Unfortunately, it also prevents storage in the adrenals and gonads
- Research to identify selective ACAT inhibitors – an arterial selective inhibitor may appear soon
- MTP (microsomal triglyceride transfer protein) inhibitors
- Mechanism of Action: Inhibits VLDL production by the liver and lowers cholesterol by preventing its exit from the liver in VLDL and LDL.
- Adverse Effects: Produces fatty liver and threat of cirrhosis.
- CETP (cholesterol ester transfer protein) inhibitors
- Mechanism of Action: Decreases reverse cholesterol transport from HDL to VLDL or IDL, thereby increasing HDL while decreasing LDL production.
- Gene Therapy – still far off
- ACAT (acyl cholesterol acyl transferase) inhibitors