
5.19: Local Flaps for Facial Reconstruction
- Page ID
- 52750

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
LOCAL FLAPS FOR FACIAL RECONSTRUCTION
Shiayin Yang, Carl Truesdale, Jeffrey Moyer
This chapter focuses on local flaps used in surgical management of cutaneous squamous (SCC) and basal cell carcinoma (BCC) of the face.
Nonmelanoma skin cancer (NMSC) is the most common type of skin cancer in the United States with an increasing annual incidence.1 Worldwide, the incidence of skin cancer is also increasing.2,3 Surgery is the most effective treatment for NMSC of the head and neck – excision or Mohs micrographic surgery (MMS). 4,5,6,7
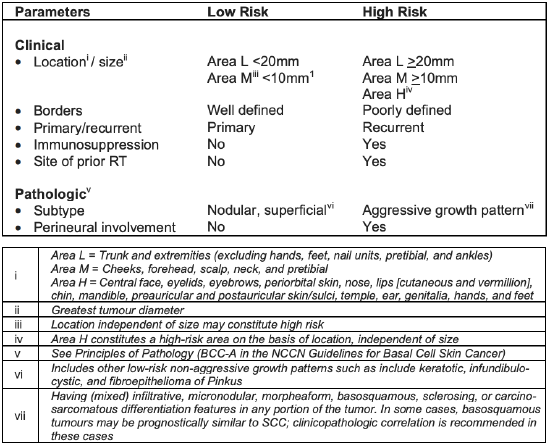
Table 1: National Comprehensive Cancer Net-work risk factors for recurrence of localised Basal Cell Skin Cancer (Adapted with permission from the NCCN Guidelines® for Basal Cell Skin Cancer V.1.2019) 5
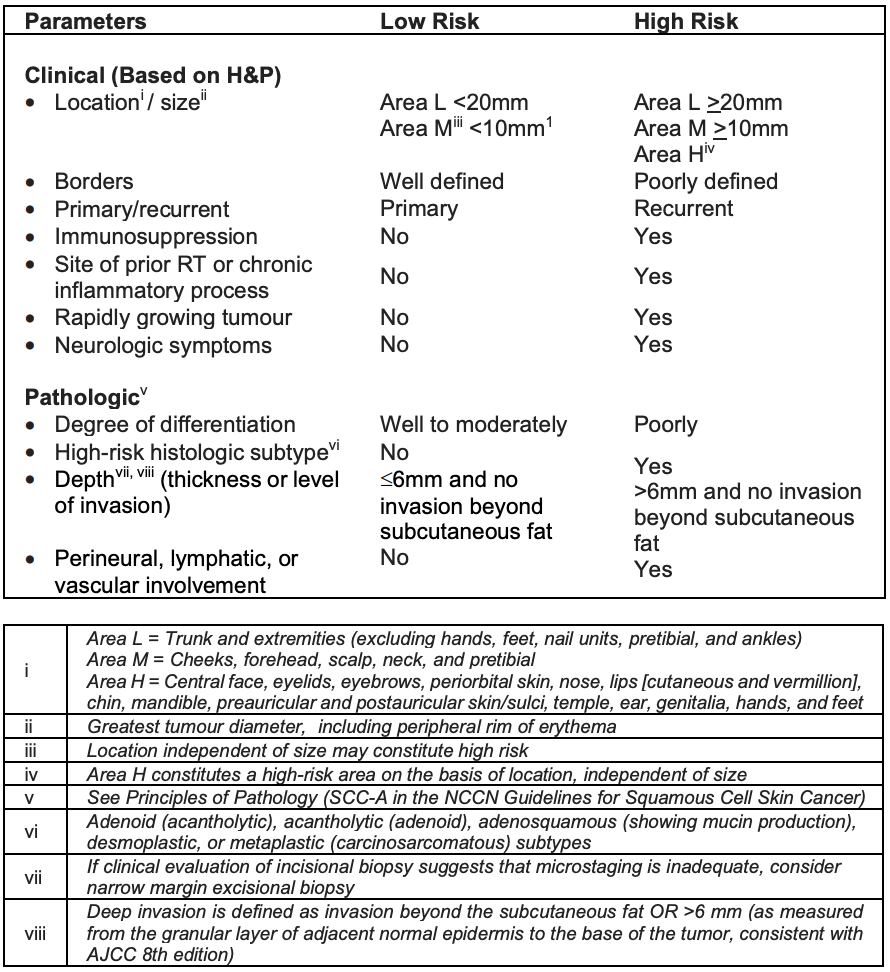
Table 2: National Comprehensive Cancer Net-work Risk Factors for Local Recurrence or Metastasis of Localized Squamous Cell Skin Cancer (Adapted with permission from the NCCN Guidelines® for Squamous Cell Skin Cancer V.2.2019) 4
Cases of local basal 4 or squamous skin cancers 5 can be divided into low- and high-risk based on clinical and pathologic characteristics (Tables 1, 2). In addition to risk of recurrence, the best treatment plan is also dependent on the type of skin cancer, location, and patient’s co-morbidities and expectations.
Standard excision
Standard excision of SCC and BCC includes excision with a margin of clinically normal appearing skin to ensure complete removal with histologically negative margins. For local low-risk SCC, standard excision of the lesion with a 4-6 mm clinical margin is a recommended option.7 For local low-risk BCC, standard excision of the lesion with a 4 mm clinical margin is recommended.6 The depth of the excision should extend into the subcutaneous tissue. The specimen should be sent for histologic assessment of the lesion and all margins. If there is concern that margins may be close or positive, then definitive reconstruction should be delayed until histologic confirmation of negative margins.
Mohs micrographic surgery (MMS)
MMS is a surgical technique that removes skin cancer with intraoperative histologic examination of 100% of surgical margins. A single surgeon excises the lesion and margins and then histologically examines the specimen. This process is repeated until the margins are negative. Clinical guidelines published by the American Academy of Dermatology recommends MMS for treatment of high-risk BCC and SCC.8
Local Flaps: Overview
A local flap comprises skin and subcutaneous tissue with a direct vascular supply, that is transferred to an adjacent or nearby site. The primary defect is the wound that is closed by the local flap; the secondary defect is the wound created after transfer of the local flap to the primary defect.
Local flaps have several advantages
- Reliable blood supply
- Good skin texture and color match
- A single stage procedure
Flaps can be defined by
- Blood supply (random or axial)
- Configuration (rhombic, bilobed)
- Location of defect (regional, interpolated)
- Type of transfer (advancement, rotation, transposition)
Choice of local flap
Determining the type of local flap to use depends on the location of the defect and the flap donor site. When planning placement and design of a local flap there are important tenets of reconstruction to bear in mind.
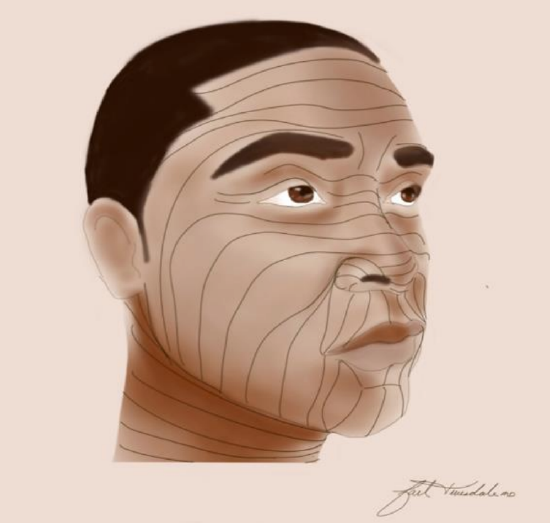
Figure 1: Incisions and closures should be planned along the relaxed skin tension lines (RSTL) which are lines of skin tension that are created from the action of underlying muscle fibers that run perpendicular to the skin
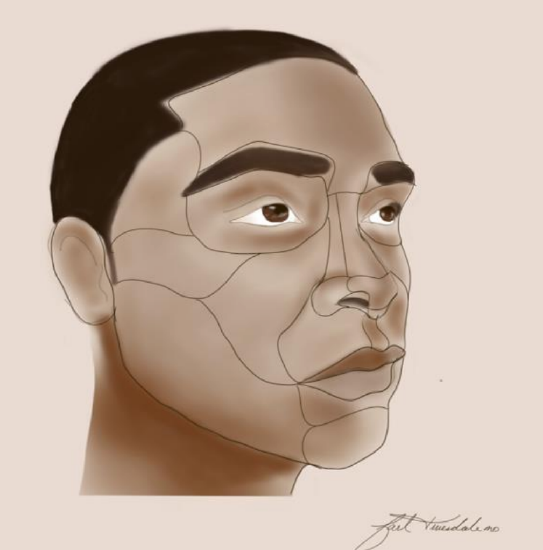
Figure 2: Illustration demonstrating aesthetic subunits of the face
- Incisions and closures should be along relaxed skin tension lines (RSTLs). RSTLs are lines of skin tension that are formed by contraction of underlying facial mimetic muscle fibers which run perpendicular to the superficial skin rhytids (Figure 1). Incisions placed along RSTLs can mimic facial rhytids and are often less conspicuous. In addition, closing along RSTLs helps to minimize tension, especially in areas that have significant aesthetic and functional value.
- Closures should be tension free. This is best accomplished by undermining the skin along the lines of maximal extensibility (LME). LME is the direction in which skin is most extensible and runs perpendicular to RSTLs and parallel to facial mimetic muscle fibers. Undermining parallel to LME allows maximal distribution of tension within the flap in order to minimize tension at the closure sites.
- Flaps should respect and preserve facial aesthetic and functional subunits (Figure 2). Placing local flap incisions along the borders of subunits can help preserve the neighboring aesthetic subunit, prevent disruption of tissue contours and function, and conceal incisions in natural shadows formed by these borders.
Advancement Flaps
Advancement flaps are flaps that slide along a linear vector to close a defect. The flap relies on stretching of tissue for advancement and is best utilized in areas of good skin elasticity. The point of greatest wound tension is at the distal border of the flap. Advancement flaps include unipedicle, bipedicle, and V-Y flaps.
Unipedicle advancement flaps
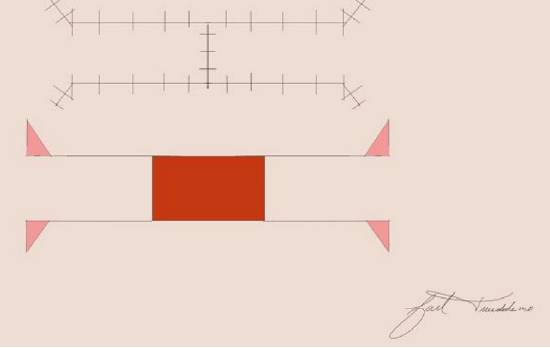
Figure 3: H-plasty
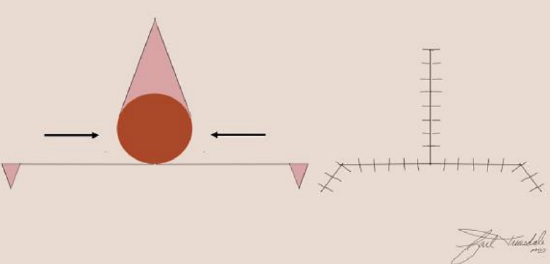
Figure 4: O-to-T flap
A unipedicle advancement flap shares a border with its defect and is advanced in a linear direction over the defect. The border between the defect and the flap becomes the leading edge of the advancement flap. As the flap is advanced, standing cutaneous deformities develop on either side of the flap’s base and can be excised with Burrow’s triangles. Bilateral unipedicle advancement flaps can be used to close larger defects by placing the flaps on opposing sides of the defect and advanced towards each other. The resulting shape of wound closure from bilateral unipedicle flaps is referred to as an H- or a T-plasty (Figures 3, 4).
Note how H- and O-to-T-plasty advancement flaps utilize two opposing unipedicle flaps to close a primary defect. Burrow’s triangles are removed at the base of the flap to correct standing cutaneous deformities.

Figure 5a: A 1.5 cm circular defect of the left cheek. Standing cutaneous deformities marked on the superior and inferior border of the defect

Figure 5b: Bilateral unipedicle advancement flaps used to close defect
H or O-to-T advancement flaps are employed in areas where minimal tissue distortion is imperative such as near the eyebrow, helical rim, and vermilion border. They can also be used to close defects of the cheek, temple, and forehead (Figures 5ab).
Bipedicle Advancement Flap
A bipedicle advancement flap advances tissue at a right angle to the linear axis of the flap to close an adjacent defect. The flap is designed to be longer than the defect and with a width equal or slightly greater than that of the defect. A secondary defect is produced with closure of the primary defect and requires closure with a skin graft. Given the creation of a secondary defect, bipedicle advancement flaps are often reserved for repair of large scalp defects and small full thickness nasal defects. A common bipedicle advancement flap involves the vestibular mucosa to repair full-thickness defects of the alae where the mucosa is pedicled medially and laterally. The secondary defect created by the advancement is repaired with a full-thickness skin graft to prevent contraction.
V-Y Advancement Flap
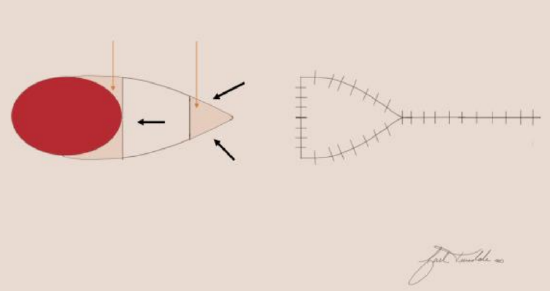
Figure 6: V-Y advancement flap with original configuration in the shape of a V. The flap is advanced in a linear direction while maintaining a subcutaneous pedicle that is at least 1/3 the length of the flap. With closure of the flap, the final configuration is Y-shaped
The V-Y advancement flap relies on a subcutaneous pedicle to supply an island of skin that is advanced in a linear direction to close a defect (Figure 6).

Figure 7a: 2 cm skin defect of the upper lip involving the vermillion border

Figure 7b: V-Y advancement flap design with borders along the vermilion border and melolabial crease

Figure 7c: Flap in position after advancement with a final Y-shaped configuration
The flap is designed in a triangular fashion with the leading edge designed to be of similar size to the defect, and the sides parallel to RSTLs or within natural creases or folds. The flap is incised along all edges down to subcutaneous tissue. The surrounding tissue is undermined away from the pedicle to allow for flap mobilization. The leading and tail edges of the flap can be undermined provided that at least 1/3 of the flap is in continuity with the pedicle to ensure adequate blood supply. Closure of the wound forms a Y configuration (Figures 7a-c). The maximum point of wound tension is at the apex of the flap. This flap is used to repair defects of the lip, cheek, forehead, and nose.
Rotation Flaps
Rotation flaps are pivotal flaps that recruit adjacent tissue to close a primary defect.

Figure 8a: Planned left cheek defect marked with blue sutures. Design of rotation flap, recruiting skin from lateral cheek. Burrow’s triangle marked on inferior aspect of planned check defect to account for correction of standing cutaneous deformity after flap rotation. Arrow indicates direction of flap rotation

Figure 8b: Flap inset. Standing cutaneous deformity removed with inset along nasolabial crease
They are versatile flaps and are best utilized to close triangular-shaped primary defects. The flap is designed in a curvilinear fashion with the defect forming a portion of the flap’s arc of rotation. It is best to base the flap inferiorly and medially and bordering a RTSL. The length of the flap should be about four times the width of the triangular defect. The point of greatest wound tension is at the apex of the flap. Rotation of the flap causes a standing cutaneous deformity at the base of the flap, which can be corrected by excising a Burrow’s triangle. A primary defect with a height of two times the width minimizes the size of the standing cutaneous deformity. Advantages of rotation flaps include a reliable vascular supply given its broad base, and flexible design that can be placed between subunits of the face (Figures 8ab).
Rotation flaps are best suited to repair defects of the scalp but can also be used on the cheek and nose. For scalp defects, it is often helpful to employ more than one rotational flap given the inelasticity of the scalp.
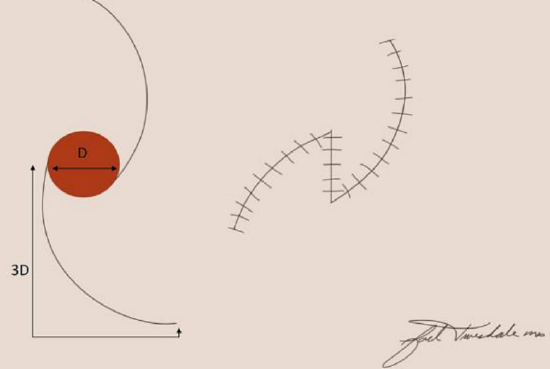
Figure 9: Two rotation flaps positioned on opposite sides of the defect. The length of the flap is three times the diameter of the defect. The final configuration after rotation of the flaps results in a Z-shape
An O-Z repair utilizes two rotational flaps, oriented on opposite sides of the defect, and pivots the flaps in the same direction to close the primary defect (Figure 9). When three rotational flaps are rotated in the same direction to close a defect this results in a pinwheel configuration.
Rotation flaps can be used for both small and large cheek defects, though they are often combined with some component of advancement. For large defects of the cheek, cervicofacial flaps are extremely reliable for reconstruction for medial and lateral defects owing to the recruitment of lateral neck skin and positioning of the scar at the borders of aesthetic subunits. For defects of the dorsum, sidewall, and tip of the nose, a dorsal nasal flap, which utilizes skin from the glabella to close defects, is a method of reconstruction.9 The dorsal nasal flap is primarily a rotation and advancement flap but also has a pivot component.
Transposition flaps
Transposition flaps are pivotal flaps with a linear configuration. The flap can share a border with the primary defect, similar to rotational flaps, but it can also be designed remotely from the primary defect. The base of a transposition flap is always contiguous with the defect. Placing the flap remotely is advantageous as the surgeon can recruit tissue from areas where there is relative skin laxity. With transposition of the flap, a standing cutaneous deformity is formed at the base of the flap. Excision of the standing cutaneous defect should be away from the base of the flap so not to compromise the flap’s blood supply. The area of greatest wound closure tension is at the closure site of the secondary defect. Transposition flaps are reliable methods of reconstruction for small and medium-sized defects of the cheek and nose. Types of transposition flaps include the note flap, bilobe flap, and rhombic flap.
Note flap
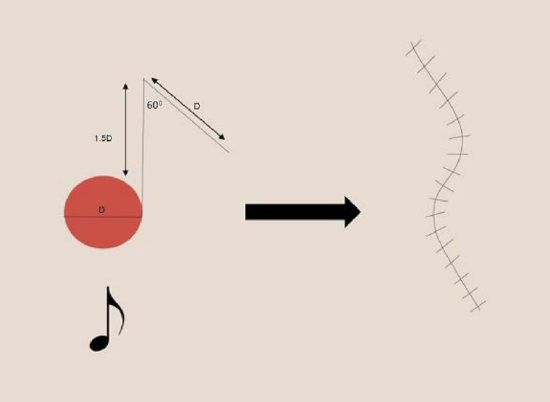
Figure 10: Transposition flap that incorporates a 60°angle triangle placed adjacent to the defect. The flap resembles a musical eighth note
The note flap is a transposition flap designed as a triangle with 50-60° degree angle used to close an adjacent circular defect.10 The flap is named for its design, which resembles a musical eighth note (Figure 10). The limb of the flap adjacent to the defect has a length of 1.5 times the diameter of the defect and is drawn parallel to a RSTL. The second limb of the flap is equal to the diameter of the defect. The triangular flap is transposed to close the primary defect, and the distal tip of the defect is trimmed as needed. The donor site is closed primarily (Figure 10).

Figure 11a: Skin defect of left temple

Figure 11b: Note flap design with planned tissue transposition from skin medial to defect. Burrow’s triangle marked on superior aspect of defect in order to remove standing cutaneous defect

Figure 11c: Flap inset with removal of standing cutaneous defect superiorly along temporal hairline
The greatest wound closure tension is at the point where the flap tangents the defect. It can be used to close circular defects up to 2 cm in size anywhere on the head and neck. Advantages of the note flap are its versatility, straightforward design, and ability to camouflage the donor site in natural creases or along RSTL. The main disadvantage is the need for skin laxity in order to primarily close the donor site, which limits its use to closure of small defects (Figures 11a-c).
Bilobe flap
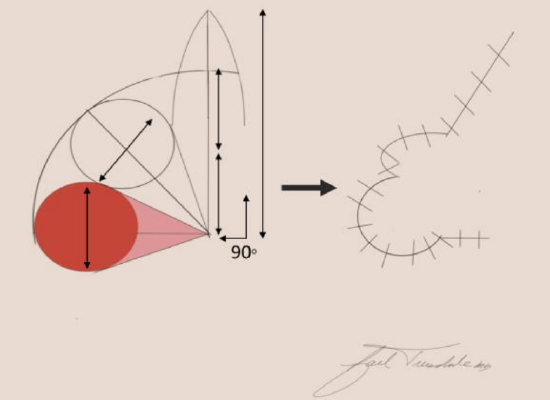
Figure 12: Bilobe flap with 90° axis of rotation. The first lobe is equal in diameter to the defect while the second lobe has a smaller diameter
The bilobe flap is a transposition flap composed of two lobes with a single base around which the flap pivots. The flap was first described with an arc of rotation of 180° with axes of 90° between the defect and 1st lobe as well as between the 1st and 2nd lobes.11 The flap has undergone modifications by limiting the arc of rotation to 90° to decrease the size of the standing cutaneous deformities and decrease trapdoor deformity (Figure 12).12
Placement of the flap should be in an area of greater skin elasticity to allow for adequate tissue recruitment.

Figure 13a: Skin defect of nasal tip

Figure 13b: Design of bilobe flap extending over nasal dorsum with Burrow’s triangle marked on the lateral aspect of the defect

Figure 13c: The bilobe flap inset with removal of standing cutaneous deformity
Bilobe flaps are most commonly employed for the caudal one-third of the nose, but they can also be a good reconstructive option for large cheek defects. The primary lobe of the flap is designed to be of similar surface area and adjacent to the primary defect. For cheek defects, the primary lobe may be up to 25% less than the defect size due to the relative increased skin elasticity of the cheek compared to the nose. The size of the secondary lobe is typically smaller than that of the primary lobe (50-100% the size of the primary lobe) and is closed primarily by skin advancement. The main advantage of the bilobe flap is the ability to recruit skin from a distal site where skin redundancy allows primary closure of the tertiary defect (Figures 13a-c). The major disadvantages of the flap are the large scar, the tendency for trapdoor deformity, especially in patients with thick sebaceous skin, and difficulty placing the incisions parallel to RSTL due to the complex design.
Rhombic (Limberg) flap

Figure 14: Rhombic flap with internal angles of 60 and 120°
The classic rhombic (Limberg) flap is a transposition flap used to repair defects in the shape of a rhombus with internal angles of 60° and 120°.13 A rhombus in this configuration can also be thought of as two equilateral triangles; thus all sides of the rhombus are of equal length. If a cutaneous defect does not have a 60°-120° rhombus configuration then additional skin can be removed to create this configuration. The 1st side of the flap is designed by extending a line equal to the length of a short diagonal, which bisects one of the 120° internal angles. The 2nd side is made parallel to the adjacent side of the rhombus and is of equal length to the 1st side. The flap is then transferred by both pivotal and advancement movement with the point of greatest wound tension at the donor site (Figure 14).
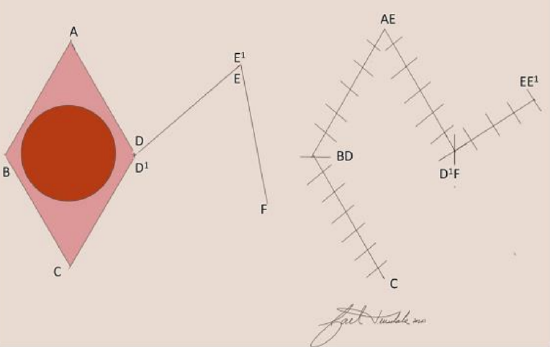
Figure 15: Modification of Limberg rhombic flap with internal angles less than 60 and 120°

Figure 16a: Right temple lesion planned for excision

Figure 16b: Dufourmentel rhombic flap designed on the inferior border of the planned defect
The rhombic flap is versatile and can be used to repair defects of the cheek, temple, chin, and neck. Advantages include minimal tissue distortion, predictable scars, and lower likelihood of trapdoor deformity. Disadvantages are formation of standing cutaneous deformity, need to excise normal skin to create a rhombic defect, and that a portion of the scar does not lie within the RSTL. The Dufourmentel flap is a modification of the classic rhombic flap and can be used to close rhomboids with any combination of internal angles (Figure 15).14 The advantage of the Dufourmentel flap is a smaller standing cutaneous deformity (Figures 16ab).
Interpolated Flap
An interpolated flap is a pivot flap in which the base of the flap is not contiguous with the defect and the pedicle of the flap passes over intervening tissue in order to close the primary defect. Given that the pedicle must pass over intervening tissue, interpolated flaps routinely require a 2nd stage procedure to divide the pedicle and inset the flap. These flaps are used for tissue defects that cannot be closed with adjacent flaps due to insufficient tissue or skin laxity. The paramedian forehead and melolabial flaps are interpolated flaps that can be used to reconstruct nasal defects.
Paramedian Forehead Flap (Figures 17ad, 18)

Figure 17a: Lateral view of skin defect involving right nasal tip and soft tissue triangle. Nasal subunits involving the defect and adjacent to defect outlined

Figure 17b: Bird’s eye view of skin defect and outlined nasal subunits of right tip and ala

Figure 17c: Lateral view of paramedian forehead flap inset with reconstruction of right hemi-tip

Figure 17d: Bird’s eye view of paramedian forehead flap inset

Figure 18a: Subtotal nasal defect of nasal dorsum, tip, columella, both alae and soft tissue triangles. Right paramedian forehead flap designed over supratrochlear artery

Figure 18b: Bird’s eye view of paramedian forehead flap after inset with pedicle attached

Figure 18c: Basal view of nasal defect with grafted cartilage to reconstruct the nasal framework

Figure 18d: Basal view after inset of paramedian forehead flap
The paramedian forehead flap is an interpolated flap with an axial blood supply provided by the supratrochlear artery and with some contributions from the supraorbital artery. It is designed over the path of the supratrochlear artery. The supratrochlear artery exits the orbit 1.7 to 2.2 cm lateral to midline, which roughly corresponds to the medial eyebrow. At this level the artery travels under the orbicularis oculi and over the corrugator supercilia. The artery then pierces the orbicularis and frontalis muscles to travel more superficial in the cephalic direction. Due to its reliable blood supply, the length of the flap can be 4 times the width of the pedicle.
There are many reasons why the paramedian forehead flap is the workhorse in reconstruction of large nasal defects – it provides significant tissue for coverage; has a similar skin color and texture to the nose; and it can revascularize cartilage or bone grafts needed to reconstruct the nose.
When planning the design of the flap, it is important to evaluate the nasal skin defect and the nasal subunits involved. If the defect involves more than 50% of a subunit, the entire subunit should be excised and reconstructed. A template is made of the defect and the excised subunits. This template is placed just below the hairline along the course of the supratrochlear artery. If the template is large or more skin/pedicle length is needed, then the template can be placed within the hair with the understanding that hair removal from the flap will be needed postoperatively.
Cephalically, the flap is raised in a subcutaneous plane, which allows for a thin and pliable flap that can easily be contoured to the nasal defect. If more bulk is needed to cover a deep defect, then frontalis muscle can be left on the flap. As dissection proceeds caudally, the course of the artery is deeper and thus dissection should be below the fascia or periosteum to protect the pedicle. The flap is inset into the nasal defect after structural grafting has been undertaken. A full thickness skin graft taken from the supraclavicular fossa can be sewn to the open portion of the pedicle to reduce postoperative oozing. The donor site is closed primarily. If the donor site is too large to be closed primarily, portions can be left to granulate with adequate aesthetic outcomes.
The forehead flap remains attached for approximately 3 weeks to the recipient and donor sites via the skin pedicle containing the supratrochlear artery. After 3 weeks, sufficient blood supply has developed from the periphery of the recipient site, and the vascular pedicle may be safely divided and the recipient and donor sites aesthetically repaired.
After detachment and inset, additional procedures, can be performed to thin and contour the flap as needed.
The main disadvantages of paramedian forehead flaps are the need for at least 2 procedures, a large donor site scar, potential for alopecia at the donor site, and greater risk of postoperative bleeding compared to other local flaps.
Melolabial Flap

Figure 19a: Skin defect involving left nasal tip, soft tissue triangle, and ala. Melolabial flap designed along melolabial groove. Asterisk marks the pedicle of the flap to be kept intact. Double asterisks mark the skin flap to be transposed onto the defect

Figure 19b: Melolabial flap inset with pedicle intact. The pedicle is taken down 3 weeks later and the lateral aspect of the flap is inset. Asterisk marks pedicle of flap
The melolabial flap is an interpolated flap that transfers tissue from the cheek to reconstruct nasal ala defects. The flap is designed lateral to the melolabial crease. Given the inherent redundancy of tissue in this area, there is usually enough tissue for flap transfer and primary closure of the donor site. The blood supply can be based on cutaneous or subcutaneous pedicles. Advantages of the flap are its ability to recruit tissue from an area with increased skin elasticity, and redundancy and ease of scar camouflage within the melolabial crease. The main disadvantage is the need for a second stage procedure to take down the pedicle (Figure 19).
Abbe Flap

Figure 20ab: Abbe flap used to reconstruct the lower lip
The Abbe flap is an interpolated flap used to repair full thickness lip defects that comprise >25% of the lip and cannot be closed primarily or with advancement flaps. The flap is designed from the opposing lip with the height of the flap equal to that of the defect and the width about half the width of the defect (Figures 20ab). The labial artery serves as the vascular pedicle and runs between the orbicularis oris and lip mucosa. Once the flap has been designed, it is raised with preservation of the labial artery and pivoted almost 180° into the defect. Inset of the flap requires special attention to reapproximate the vermillion border and the mucosa, muscle, and skin. The secondary defect is closed primarily. While the pedicle is attached, patients consume a liquid and soft diet to limit strain on the pedicle. The pedicle of the flap is divided after 3 weeks and the flap is fully inset.
Postauricular Flap

Figure 21a: Skin and cartilage defect of helical rim and scapha

Figure 21b: Conchal cartilage graft used to reconstruct scapha and portion of helical rim

Figure 21c: Postauricular skin flap inset over cartilage framework
The postauricular flap is a two-stage procedure used to reconstruct large defects of the auricle that require both cartilage and soft tissue repair. The first stage involves reconstruction of the cartilaginous framework and a posteriorly based cutaneous advancement flap. The flap is elevated from the medial aspect of the auricular defect and continued posteriorly into the postauricular sulcus and onto the scalp. The width of the flap is equal to the height of the defect. Once the flap is elevated, the cartilaginous framework is reconstructed using harvested conchal or septal cartilage. The cartilaginous framework is laid underneath the flap and the flap is secured to the skin on the anterior aspect of the defect, in order to completely cover the cartilage. The advancement flap remains attached for 3 weeks. At the 2nd stage, the advancement flap is released from the scalp and used to cover the medial aspect of the defect. A skin graft is used to repair the secondary defect from the advancement flap (Figures 21a-c).
References
- Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence Estimate of Nonmelanoma Skin Cancer (Keratinocyte Carcinomas) in the U.S. Population, 2012. JAMA Dermatol. 2015; 151(10):1081-6
- Leiter U, Eigentler T, Garbe C. Epidemiology of skin cancer. Adv Exp Med Biol. 2014;810:120-40
- Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7(2):1-6
- National Comprehensive Cancer Center. NCCN clinical practice guidelines in oncology; squamous cell skin cancer (V2.2019). Available at: www.nccn. org. Accessed June 17, 2019
- National Comprehensive Cancer Center. NCCN clinical practice guidelines in oncology; basal cell skin cancer (V1.2019). Available at: www.nccn.- org. Accessed June 17, 2019
- Kim JYS, Kozlow JH, Mittal B, et al. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540-59
- Kim JYS, Kozlow JH, Mittal B, et al. Guidelines of care for the management of cutaneous squamous cell carcinoma. J Am Acad Dermatol. 2018;78(3):560- 78
- Connolly SM, Baker DR, Coldiron BM, et al. AAD/ACMS/ASDSA/ASMS 2012 appropriate use criteria for Mohs micrographic surgery: a report of the American Academy of Dermatology, American College of Mohs Surgery, American Society for Dermatologic Surgery Association, and the American Society for Mohs Surgery. J Am Acad Dermatol. 2012;67(4):531-50
- Rieger RA. A local flap for repair of the nasal tip. Plast Reconstr Surg. 1967;40 (2):147-9
- Walike JW, Larrabee WF. The 'note flap'. Arch Otolaryngol. 1985;111(7): 430-3
- Esser JFS. Gestielte lokale Nasenplastik mit zweizipfligem Lappen, Deckung des sekundaren Defektes vom ertsen Zipfel durch den zweiten. In. Vol 143. Deutsche Zeitschrift für Chirurgie 1918:385-90
- Zitelli JA. The bilobed flap for nasal reconstruction. Arch Dermatol. 1989; 125(7):957-9
- Limberg AA. Modern trends in plastic surgery. Design of local flaps. Mod Trends Plast Surg. 1966;2:38-61
- Dufourmentel C. [Closure of limited loss of cutaneous substance. So-called "LLL" diamond-shaped L rotationflap]. Ann Chir Plast. 1962;7:60-6
Other flaps described in The Open Access Atlas of Otolaryngology Head & Neck Operative Surgery
- Pectoralis major flap
- Buccinator myomucosal flap
- Buccal fat pad flap
- Nasolabial flap
- Temporalis muscle flap
- Deltopectoral flap
- Paramedian forehead flap
- Upper and lower trapezius flaps
- Cervicofacial flaps
- Submental artery island flap
- Supraclavicular flap
- Latissimus dorsi flap
- Radial free forearm flap
- Free fibula flap
- Rectus abdominis flap
- Anterolateral free thigh flap
- Thoracodorsal artery scapular tip (TDAST) flap
- Principles and technique of microvascular anastomosis for free tissue transfer flaps in head and neck reconstructive surgery
Also refer to Open Access chapter: Surgical management of skin cancers of the head and neck
Authors
Shiayin F. Yang MD
Center for Facial Cosmetic Surgery
University of Michigan
19900 Haggerty Rd; Suite 103
Livonia, MI 48152
shi1yang@gmail.com
Carl Truesdale MD
Center for Facial Cosmetic Surgery
University of Michigan
19900 Haggerty Rd; Suite 103
Livonia, MI 48152
ctruesda@med.umich.edu
Jeffrey S. Moyer, MD
Center for Facial Cosmetic Surgery
University of Michigan
19900 Haggerty Rd; Suite 103
Livonia, MI 48152
jmoyer@med.umich.edu
Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za